Cranial Nerves
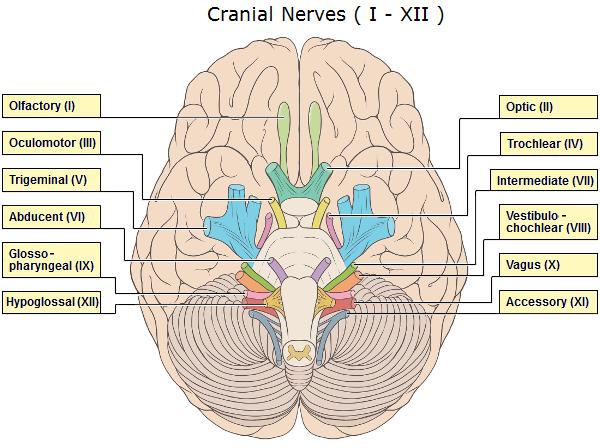
I. Olfactory Nerve
The origin is the Olfactory bulb and it has the special sensory function of smell. Problems with the Olfactory Nerve can result in anosmia, which is the loss of the sense of smell.
II. Optic Nerve
The origin is the Thalamus and it has the special sensory function of vision. Problems with CN II can result in loss of vision.
III. Oculomotor Nerve
The origin is the Midbrain, and it has a motor and parasympathetic function. The motor function moves the eyes left and right and controls the eyelid. The parasympathetic function controls pupil constriction. Problems with CN III can result in a loss of pupillary light reflex, papilledema and ptosis.
IV. Trochlear Nerve
The origin is the Midbrain, and it has the motor function of moving the eyes up and down. Problems with CN IV can result in diplopia, nystagmus, and difficulty moving eyes up and down.
V. Trigeminal Nerve
The origin is the Pons, and it has a sensory and motor function. The sensory function controls touch, pain, temperature & vibration for face, mouth, and anterior 2/3 of tongue. The motor function controls chewing muscles. Problems with CN V can result in a loss of the previously mentioned sensations, difficulty chewing, and an abnormal jaw- jerk reflex.
VI. Abducens Nerve
The origin is the Pons, and it has a motor function of rotating the eyes out. Problems with CN VI can result in strabismus, where the eye rotates in, diplopia and nystagmus.
VII. Facial Nerve
The origin is the Pons, and it has motor, sensory, special sensory and parasympathetic functions. The motor function controls the muscles of the face. The sensory function controls the sensation near the ears. The special sensory function controls taste in the anterior 2/3 of the tongue. The parasympathetic controls the salivary glands. Problems with CN VII can result in facial paralysis/ paresis or taste loss.
VIII. Vestibulocochlear Nerve
It is also known as the auditory nerve. It originates at the Pons/Medulla junction and has a special sensory function controlling hearing and balance. Problems with CN VIII can result in hearing loss or balance problems.
IX. Glossopharyngeal Nerve
The origin is the Pons/Medulla junction, and it has motor, parasympathetic, sensory and special sensory functions. The motor function controls pharyngeal movement. The parasympathetic function controls the parotid gland (salivation). The sensory function controls the middle ear, pharynx, and posterior 1/3 of the tongue. The special sensory function controls taste on the posterior 1/3 of the tongue. Problems with CN IX can result in an absent gag and swallow reflex, loss of taste, and loss of pharyngeal movement.
X. Vagus Nerve
The origin is the Medulla and it has motor, parasympathetic, sensory and special sensory functions. The motor function controls pharyngeal and laryngeal muscles. The parasympathetic function controls the heart, lungs and digestive tract. The sensory function controls the pharynx and blood pressure, and the special sensory controls taste from epiglottis and pharynx. Problems in CN X can result in absent gag and swallow reflex, loss of velar movement or loss of voice.
XI. Spinal Accessory Nerve
The origin is the Medulla and Spinal Cord, and it has a motor function which controls the neck and shoulder muscles. Problems in CN XI can result in droopy shoulder, or difficulties with movement of the neck.
XII. Hypoglossal Nerve
The origin is the Medulla, and the function is motor control of muscles of the tongue. Problems with CN XII can result in loss of tongue movement; tongue fasciculations, and tongue atrophy.
The most important nerves for speech and hearing are CN V, VII, VIII, IX, X, XII.
